
 PARENTING TIPS
PARENTING TIPS PREGNANCY
PREGNANCY BABY CARE
BABY CARE TODDLERS
TODDLERS TEENS
TEENS HEALTH CARE
HEALTH CARE ACTIVITIES & CRAFTS
ACTIVITIES & CRAFTS
Many pregnant women know that the baby should be head down to have a safe and successful vaginal delivery. I remember panicking during my pregnancy because my little one was breech at 28 weeks, and I hoped to avoid a C-section. I did tons of research and interventions on how to flip a breech baby naturally, from chiropractic care and headstands to essential oils. While there was plenty of time for her to flip before delivery, I knew her breech position could compromise my goals for a natural birth.
I did not know that even if a baby’s head is down, other aspects of fetal positioning can also affect delivery outcomes. One of these is the posterior position. While it is possible to have a vaginal birth with a posterior baby—and many women do—it is not optimal. So, what does it mean if your baby is posterior, why does it matter, and how can you turn them naturally?
What is a Posterior Baby?
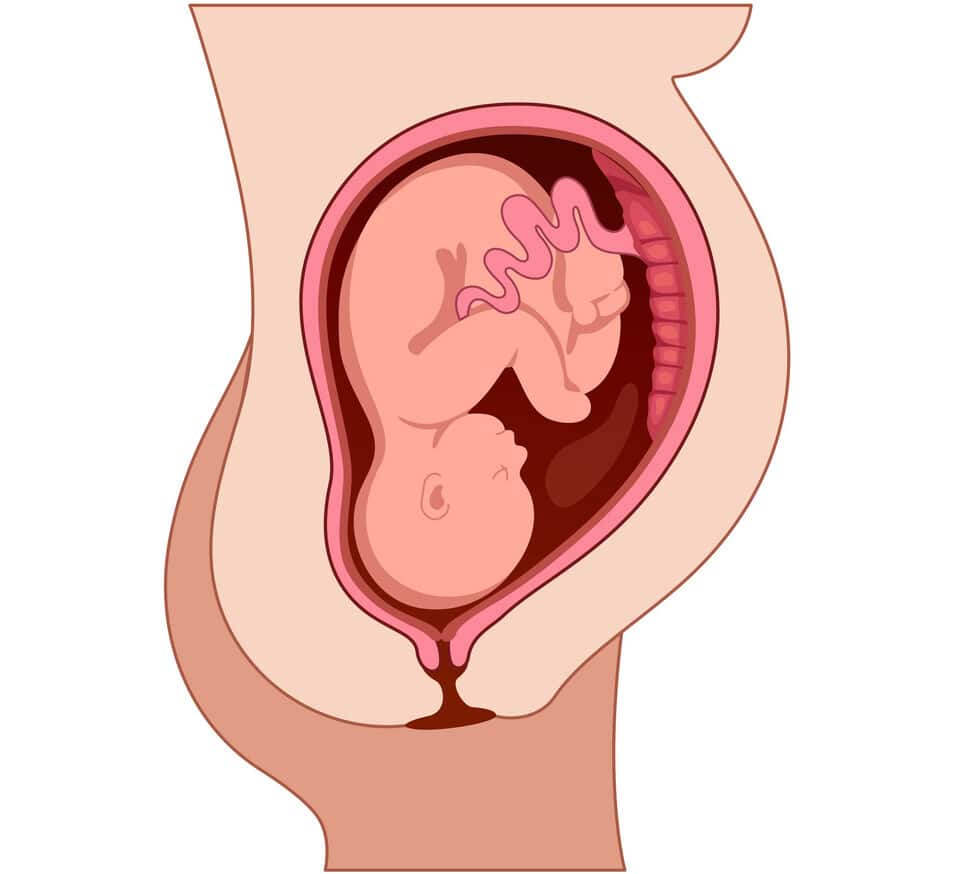
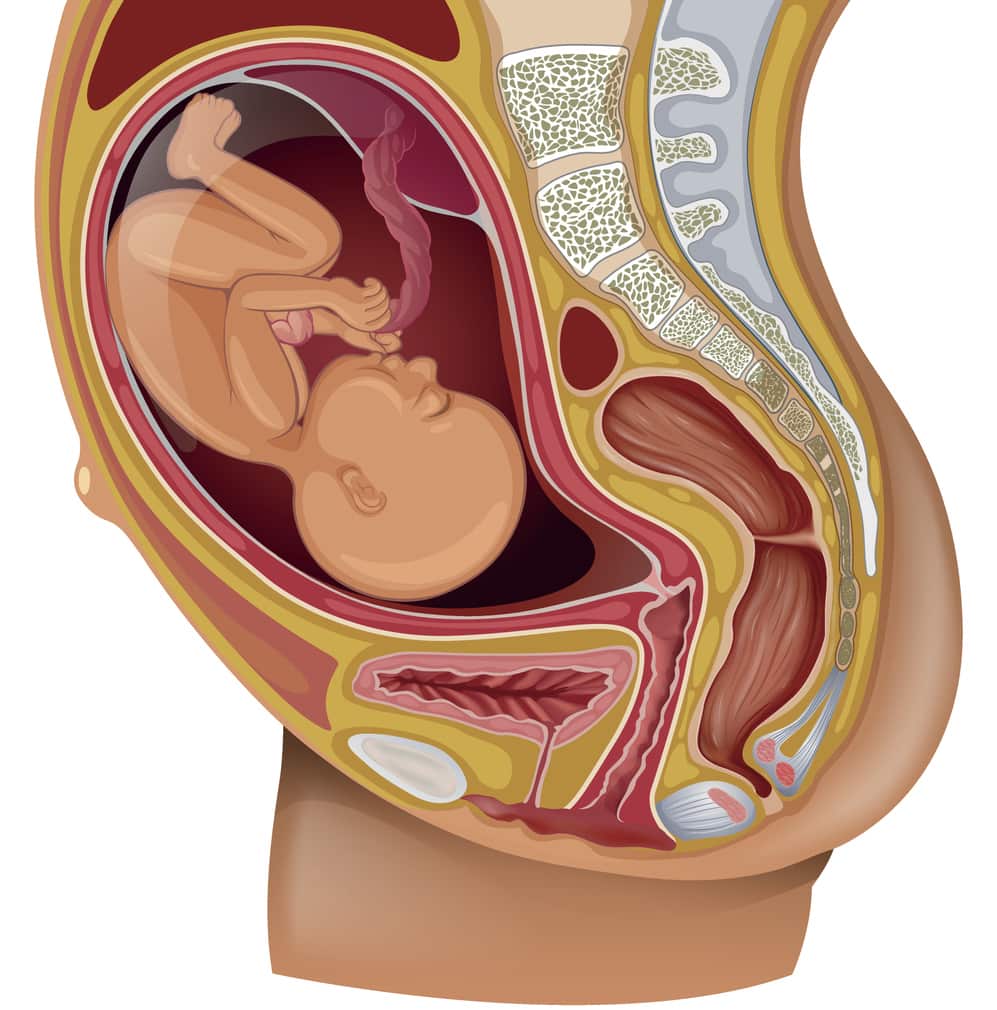
The full medical term for a posterior baby is “fetal occiput posterior,” which means the back of the baby’s head (occiput) is toward the mother’s back (posterior). In other words, the baby’s spine is to mother’s spine.1
You may have heard a posterior baby referred to as “sunny-side up.” This is because if a mother births on her back, the baby will be face-up when they come out of the birth canal. The baby’s face, its “sunny side,” is facing up.
How Common is the Posterior Position for a Baby?
Between 15% and 32% of babies are posterior when labor begins. When your cervix fully dilates, and it is time for delivery, the likelihood that your baby is still posterior is between 1.8% and 12.9%. Since many babies rotate independently during labor, posterior babies are more common in the earlier stages.2,3
Why Does the Posterior Position Matter?
The best fetal position for birth is called occiput anterior, meaning the baby is facing the mother’s back. It’s when the crown of the baby’s head emerges first through the dilated cervix, and the chin is likely flexing toward the chest. This position minimizes the diameter of the baby’s head, allowing it to fit optimally through the mother’s pelvis and birth canal.3
When a baby is posterior or faces forward, the presenting part of the head is larger. This can make labor and delivery longer and more complex.
Risks of Having a Posterior Baby
There are risks to the mother and the baby when laboring with and delivering a posterior baby.3
Risks to the mother include the following:
- Longer labor
- Increased likelihood of labor augmentation
- C-section
- Worsened tearing
- Hemorrhage
Risks to the baby include:
Many of the risks to a posterior baby are related to the fact that the baby’s positioning often causes more prolonged labor.4
Who is Likely to Have a Posterior Baby?
The following groups are more likely to have a posterior baby whose position persists through delivery:3
- First-time mothers
- Black mothers
- Moms older than 35
- Moms of shorter height
- Moms whose labor was induced or augmented with Pitocin
- Moms with an anterior placenta
- Babies past their due date
- Large babies
How Do I Know If My Baby is Posterior?
Back Labor
Back labor refers to pain in your lower back during labor contractions. It may persist between contractions, whereas uterine pain is relieved between contractions. Back labor is worse when a baby is posterior because the back of the baby’s head pushes on your spine and tailbone. If you experience back labor, you can be suspicious that your baby is in the posterior position.2,5
Leopold’s Maneuvers
Your provider may perform hand movements on your abdomen to identify which part of your baby’s body is presenting at each part of your uterus. Your provider’s experience, your baby’s gestational age, and body mass can all affect the accuracy of these maneuvers for identifying fetal position and orientation.6
Digital Vaginal Examination
During a vaginal exam, your provider may be able to feel the soft spots or fontanelles on your baby’s head. This can help identify the orientation of the baby’s head and tell whether your baby is posterior. This method of determining the baby’s position is often inaccurate but more likely accurate with more experienced providers, if the cervix is more dilated, and if the baby is more descended.3,5
Ultrasound
Ultrasound is the superior method of confirming a baby’s position during labor. Depending on your baby’s height, a doctor can perform an ultrasound on your abdomen, through your vagina, or on your perineum. If you are giving birth in a hospital, most labor and delivery units have a portable ultrasound machine to observe a baby’s position quickly.5,3
How to Naturally Turn Your Posterior Baby
Gravity
A baby’s head and back are the densest parts of their bodies. Any maternal position that makes her belly into a hammock allows the heavy back of the baby to rotate toward the mother’s front. Forward-leaning positions also make the uterus larger and rounder, leaving more room for the baby to rotate.4
Examples of forward-leaning labor positions that work with gravity to rotate your baby include:2,4
- All fours or hands and knees
- Standing while leaning forward and resting hands on a bed, wall, or ball
- Straddling an armless chair backward and resting arms and head on the back of the chair
Pelvic Rocking
Pelvic rocking, or pelvic tilts, also uses gravity and can effectively encourage your baby to rotate its back toward your front.4
For pelvic tilts, get on the floor or bed on all fours and alternate arching your back to the sky and the ground. Crawling on your hands and knees across the floor can mimic this pelvic movement and allow your baby to rotate.2
Rebozo
While there are no formal studies on its efficacy, a rebozo, or a Mexican woven shawl, has a rich history and tradition of repositioning a fetus. It can also provide physical relief and comfort to a mother during labor. There have been anecdotal reports and case studies of rebozo work helping to get a baby into the best position for delivery.
A large scarf or a folded bedsheet will also work without a rebozo. To use the rebozo technique, a laboring mother can be on her hands and knees, in a child’s pose position, or lay on her back. Depending on which position is comfortable and practical, the rebozo serves as a hammock or grip for the mom’s buttocks, hips, or belly to aid in rocking, sifting, or shimmying the baby to encourage them to rotate.7
Relaxation
Different methods of encouraging uterine and pelvic floor relaxation can allow the space and uterine positioning for your baby to rotate into the best position for birth. Some of these relaxation and repositioning methods include Webster chiropractic care and acupuncture. These can both be effective if a qualified professional performs them.8
If these natural methods of rotating your posterior baby fail, rest assured that your baby may turn spontaneously at delivery. If not, your provider may also attempt manual rotation of your baby’s head to help your vaginal delivery go more smoothly.3,5
You might learn your baby is sunny-side-up during a routine prenatal visit toward the end of your pregnancy, or you might not know until labor begins or you get admitted to the hospital. Posterior positioning is common, and while it comes with risks, your baby still has time to turn up until delivery. There are many ways you can try to rotate your baby and still achieve your birth goals, so try not to get discouraged by this news. Allow yourself as much physical and mental relaxation as possible to give your baby the best chance of turning.


